Personal Care
This page discusses my experiences with an external catheter, leg bag, internal catheter, self-catheterization, digital disimpaction, pressure sores, and a PICC line. Don’t overlook the picture gallery.
External Catheter: I use an external catheter connected to a leg bag. When applying an external catheter, make sure that no rolled up material from the catheter is left after the catheter is applied. The easiest way to do this is to unroll the catheter just a little before applying it. If you have some material left, carefully cut though the ring of material with a scissors. Don’t leave it!
Another technique I have used successfully when I notice redness is to place a Band-Aid over the area, and then apply the catheter over the Band-Aid. However, you must be extremely careful not to strangulate or impede the flow of urine with the Band-Aid. Even when not strangulating, I think the Band-Aid may affect the flow so use with caution. Also, pay close attention to the adhesive liner on the catheter and move it when necessary by allowing more or less of the catheter to unroll before applying. I also use a skin protector called Skin-Prep, which I think provides for better adhesion and protects the skin from breakdown.
Recognize that you will have catheter failures. A nuisance for sure, but as you age it becomes less embarrassing. I recommend that you just accept that it will happen. You can take a couple of steps to make this event a bit easier to manage. First, I protect the bedding with a waterproof barrier under the mattress cover. You don’t notice that it is even present. This was the only device I used for years. In the event of a failure, I still had significant washing, drying and bed making chores. About five years ago I acquiesced to my vanity and started to use a standard plastic Chux with a towel placed over the Chux. The purpose of the towel is two-fold. It absorbs the urine, and it keeps the Chux away from my skin. This system seems to work very well and minimizes the hassle when a failure occurs.
Leg Bag: I use the same leg bag day and night. At night it just lays next to my leg. I take the elastic band off my leg and remove the bottom of the bag from my sock. I rinse the leg bag daily with a 50% mixture of household bleach and water. I keep this mixture in an recycled dish soap squeeze dispenser next to the shower. Weekly I replace the bag and tube assembly.
Internal Catheter: I have used a Foley (french) catheter for brief periods as a result of a procedure or the need to stop using the external catheter due to pressure sores on the dorsal side of my penis, which wouldn’t heal. After removing the external catheter, the lesions healed completely in a very short time. The pressure sore problem has never redeveloped. I believe it is because I use the technique described above.
Self-Catheterization: From time-to-time I have had to perform catheterization. While not something most men would look forward to, it’s not too bad for me since I have no feeling in that area. My advice regarding this unusual task is to just get over it. In 1978 I was placed on a regime of self-catheterization four times a day. ITW made a neat little self-contained package (catheter and collection bag all-in-one) for this purpose. I believe it is still being made. I had an external sphincterotomy, which put a stop to the need for continuing this practice.
Digital Disimpaction: I have tried medicines, suppositories and enemas for my bowel program with zero success. Suppositories are unpredictable and slow acting. Enemas are messy and not very effective. The best technique I have found is digital disimpaction (DDI), sometimes called digital stimulation. With DDI, I use Dove soap as a lubricant and then insert my finger from my backside into my rectum. I use the finger to remove any accumulated stool. I perform this task daily while I am showering. Without any doubt this method works best for me. I suggest the rear entry versus front entry to prevent contamination and possible introduction of bacteria contained in the stool into the urinary tract. Wash your hands thoroughly before proceeding with other hygiene tasks. No special supplies are required, although I suppose you could use gloves and a water-based lubricant. Personally I don’t need more stuff to buy just to live another day.
Pressure Sores: Seek professional care immediately when pressure sores develop, especially if they are on your butt! Since my gross mismanagement of my first sores twenty years ago, I have become adept at early diagnosis and treatment. Today I treat them at home with bed rest on my waterbed. This works great. But I don’t really have trouble with pressure sores since I began using Roho cushions. Still, you must remain vigilant and examine this area frequently, if not every day.
Examining your backside is somewhat difficult, as you might imagine. Here are a few ideas that work well for me. Touch: get to know the feel of the areas on either side of your buttock, including the area around your rectum. Touching the area you will be bathing every day is a perfect first warning.
Examine your pants and bedding. They will act as sentinels and can show early spotting from a newly opened sore. The sores tend to express considerable fluid, sometimes mixed with a little blood. They leave visible spots, wet or dry. A digital camera can also be helpful; “self portraits” are easy to perform. Inspection by untrained eyes would be my last choice because sometimes these sores can be hard to see, especially for the untrained eye.
You may be able to manage some less critical sores on your own. For example, I have had recurring problems with the insides of my heels; the right heel more than the left. This hasn’t occurred as much in the last ten years. I am not certain of the cause, but it may be the result of my feet dangling all day. My shoes seem to make a huge difference. None of the fancy cures have worked, and my heel injury became chronic at one time. I would treat it according to the doctor’s instructions without improvement. Eventually I tired of this approach and settled into my own regime of washing with hydrogen peroxide straight from the bottle. A little splash over the silver-dollar-sized wound worked. Then I covered it with a 2″ x 2″ sterile gauze pad and place my sock over the pad to keep it in place. Occasionally I flood the area with provoiodine instead of peroxide. After some time the wound would heal. This care regime is what I still use today whenever needed – it’s simple and seems to work.
When admitted to the hospital I take the Roho cushion and use in bed. I place it under my butt, particularly so the ischium and tailbone are fully supported. Do not place a sheet of Chux between the cushion and you. The cushion cover is designed with a material that does not create pressure points where Chuxs will. Chuxs also trap moisture, which is never a good for your skin. This works so well that I don’t need to be turned every couple of hours. However, the nursing staff sometimes doesn’t accept that it will work. If you have problems with them, I suggest that you ask your doctor to write the appropriate order. You may want to compromise and have the nurse inspect those areas every eight hours to ensure no problems are developing.
Peripheral Inserted Central Catheter (PICC): I have had at least four PICC lines. These are central lines that are inserted into the large veins in your arm usually around the elbow. Then the catheter is threaded up your arm and down into your chest into the superior vena cava. This vein leads into the heart. The PICC insertion team verifies this placement from an X-ray before certifying the line for use.
I won’t go into boring details except for a couple of items that I have found useful. When I am preparing for bathing, I first wrap the area around the PICC with a stretch bandage. I then cover the bandage with Glad Press’n Seal plastic wrap. Don’t use Saran Warp or other imitators. You will be amazed how well Press’n Seal works. The purpose of the stretch bandage is to trap and absorb any water that get past the plastic wrap; inevitably some small amount will.
The longest I have had a PICC is for four months. I follow the sanitation directives completely and have not had any problems. I pulse (I have found nurses in the hospital often fail to perform this procedure) the saline flushes before the medicine and afterwards.
Picture Gallery
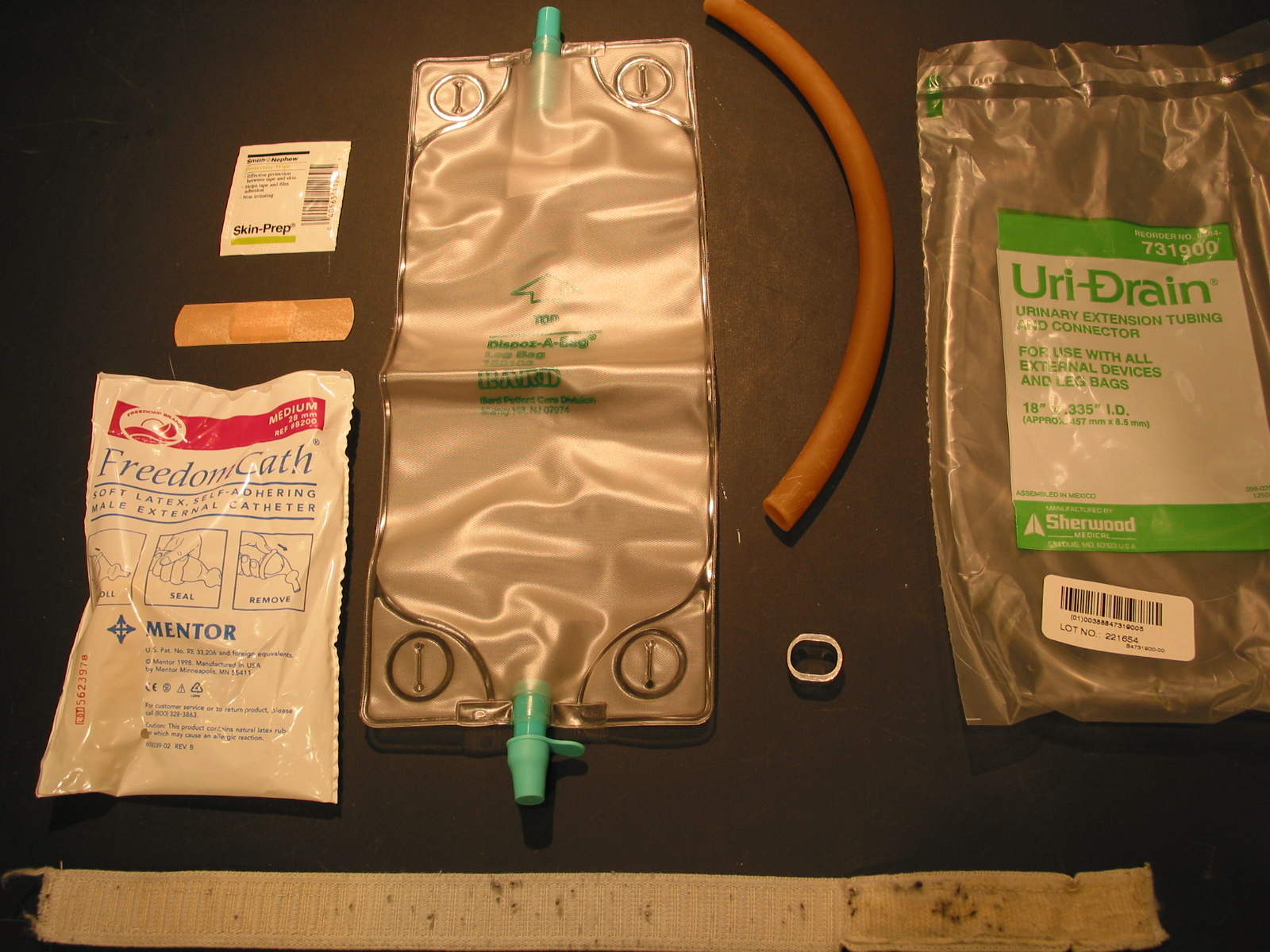
Urine collection supplies
Aluminum ring – self made, Mentor Freedom cathater, Leg bag, Elastic strap with velco clousure – self made, Skin prep, Extension tube, Latex Rubber Tubing 3/8″ ID, 1/2″ OD, 1/16″ Wall Semi-Clear Amber
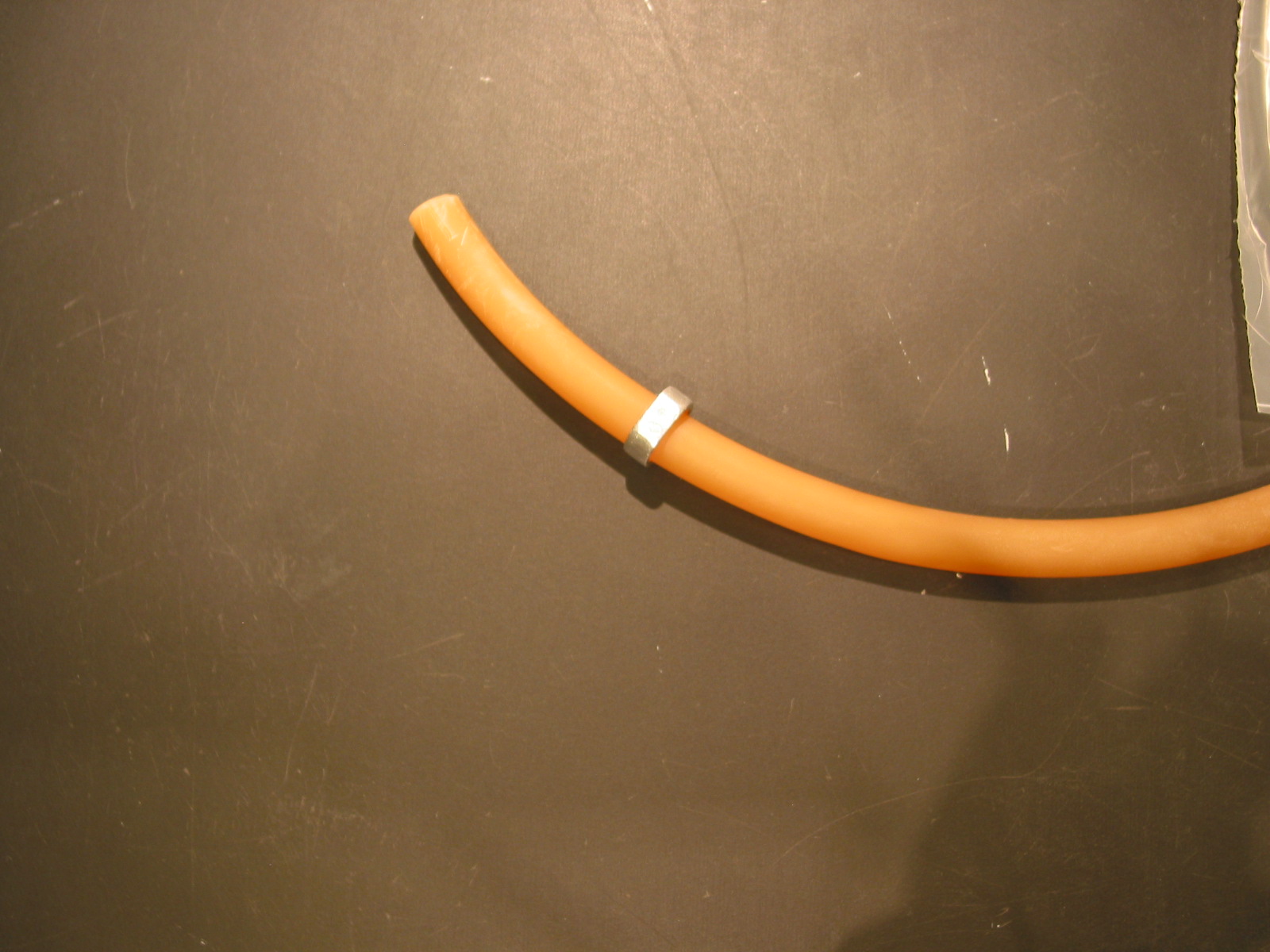
Slide ring onto tube

Bend tubing and insert through ring

Slide to bend – leaks otherwise
I prefer this solution to screw clamps becasue the ring doesn’t dig into my skin. The loose end of the bag I place into my sock.

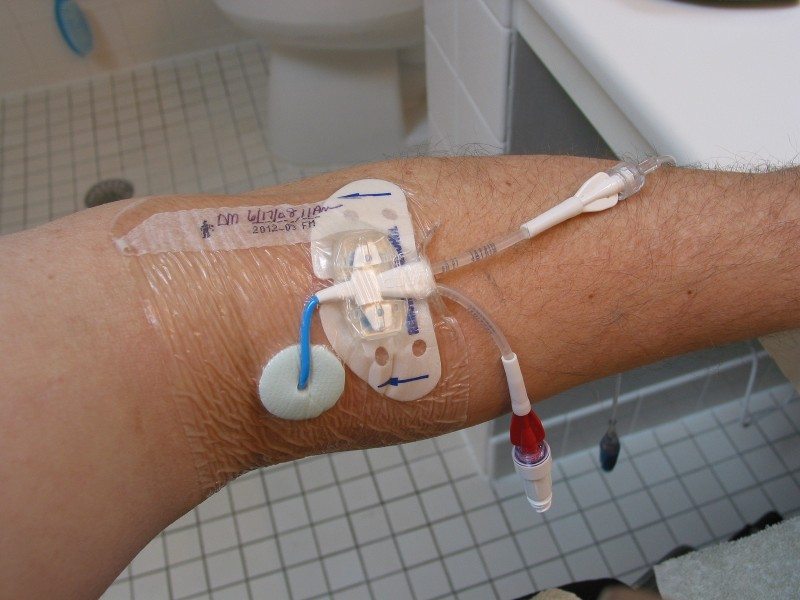
PICC line, Dressing, Statloc, BioPatch. Looks worse than it is.

Wrapped with strech bandage to prevent water from soaking though to PICC dressing.

Plastic wrap placed over the strech bandage
